Endometriosis and Cervical Stenosis
Endometriosis can affect the cervix in rare cases. But diagnosis is difficult due to the fact that cervical stenosis may be asymptomatic in nature. In some cases, endometriosis may be implicated in the diagnosis of cervical stenosis. This article is about the possible link between the 2 conditions.
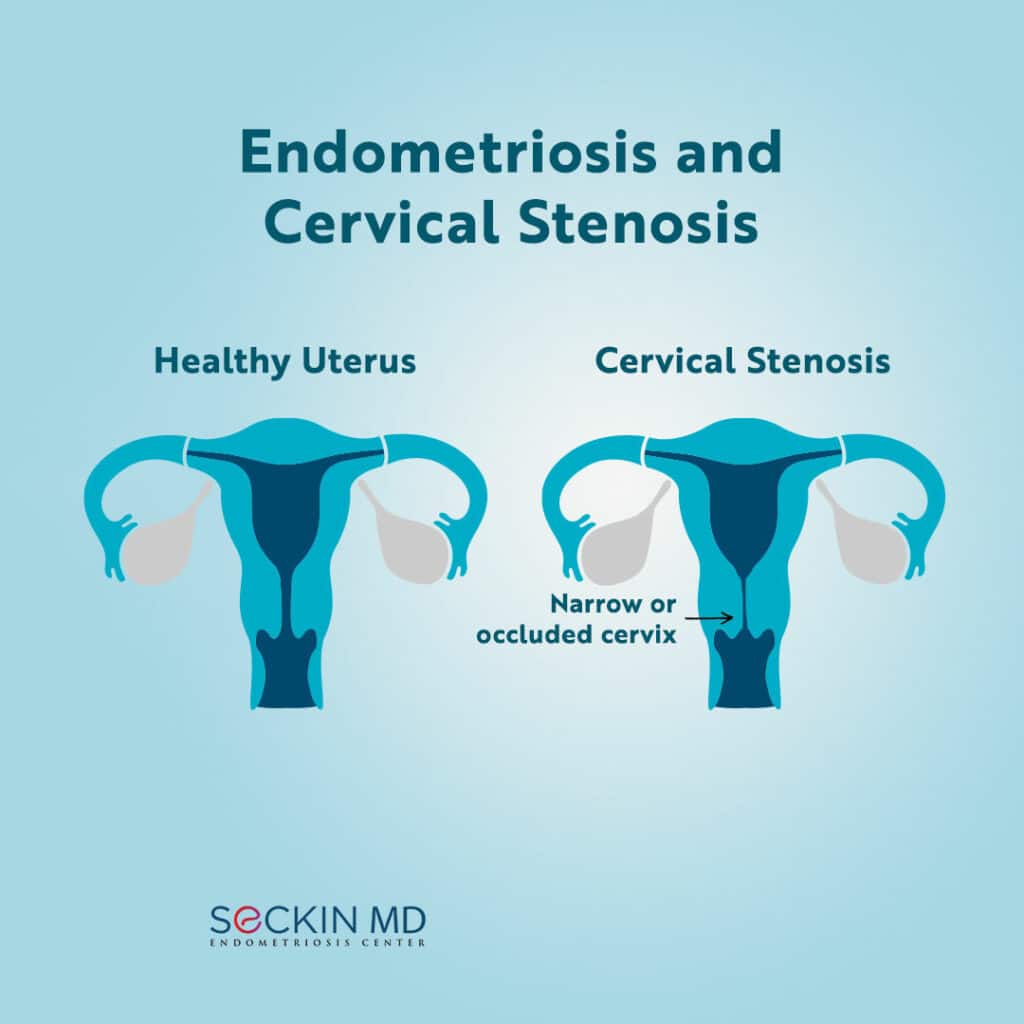
What is cervical stenosis?
The cervix is part of the uterus that is the natural opening into the vagina. Cervical stenosis refers to the narrowing of the cervical os or opening. Reasons for this include genetic abnormalities, menopause, surgical trauma to the cervix (such as cervical conization or endometrial ablation), cancer, and radiation therapy.
Cervical stenosis is usually asymptomatic, especially in postmenopausal women. However, symptoms, if present, can include dysmenorrhea, amenorrhea, bleeding, and infertility in premenopausal women.
Doctors usually diagnose cervical stenosis if a 1mm to 2mm uterine probe cannot pass through the cervix.
Is there a link between endometriosis and cervical stenosis?
There is no direct correlation between endometriosis and cervical stenosis. However, in a case study, 24 out of 25 women with chronic pelvic pain and cervical stenosis of the external cervical os also had endometriosis, based on a visual diagnosis.
Another cross-sectional study found that women with cervical stenosis of the internal cervical os and associated cervical factor infertility had a common diagnosis of endometriosis and polyps. However, a statistically significant correlation between cervical stenosis and other infertility risk factors could not be established.
Cervical stenosis and Samson’s theory of retrograde menstruation
Cervical stenosis may also explain Samson’s theory of retrograde menstruation. According to this, the menstrual effluent goes back into the reproductive tract, as there is nowhere else the blood can evacuate, leading to the increased likelihood of endometriosis forming. During hysteroscopy, surgeons typically perform cervical dilation to ease the passage of the probe through the constrained cervical opening.
Do you have cervical stenosis? Please do not hesitate to share your story if you wish by leaving a comment on our post on Facebook or Instagram.
Get a Second Opinion
Our endometriosis specialists are dedicated to providing patients with expert care. Whether you have been diagnosed or are looking to find a doctor, they are ready to help.Our office is located on 872 Fifth Avenue New York, NY 10065.
You may call us at (646) 960-3080 or have your case reviewed by clicking here.